You’ve got 20 minutes to prep tomorrow’s reading lesson. You open a worksheet site. It wants your credit card.
Or it buries the good stuff behind confusing menus. Or worst of all, the materials don’t even match your students’ reading levels.
I spent three hours testing both ReadingDuck.com and EnglishWorksheetsLand.com. I compared their organizational systems, counted their actual free resources, and measured how quickly I could find grade-appropriate materials.
One platform made my job easier. The other made me work harder. Here’s what I found when I put these two reading resource sites head-to-head.
What Each Platform Offers
ReadingDuck.com brings over 20,000 free printable worksheets focused purely on reading and literacy. No subscriptions. No sign-ups. Just instant access to materials organized in seven different methods. Research.com recently featured them on their 50 Useful Links for Learning and Teaching English for 2026: Websites, Articles, and Resources page.
The site was started by a retired reading teacher who refused to stop helping students. Other retired educators, web developers, and designers joined in. Now, it’s an entirely volunteer-run operation dedicated to fighting illiteracy.
EnglishWorksheetsLand.com claims to offer 40,000+ worksheets covering the full spectrum of English language arts. Their topics range from abbreviations and action verbs to writing prompts and vocabulary. It’s basically a one-stop shop for anything related to English instruction. The site organizes materials by topic and grade level.
The Cost Factor
Reading Duck doesn’t charge anything. Every single worksheet is free to download and print. No credit card needed. No trial periods that turn into subscriptions.
This matters more than you might think. According to the APM Research Lab, about 130 million American adults have low literacy skills. That’s 54% of adults aged 16 to 74 reading at or below a sixth-grade level. Free resources help close that gap.
English Worksheets Land’s pricing structure isn’t clearly displayed on their main website. While some materials may be accessible, the exact cost and membership requirements remain unclear unless you contact them directly.
For budget-conscious teachers and homeschool families, Reading Duck eliminates the guesswork and the expense.
Reading-Specific vs. General Language Arts
Here’s where the difference gets real. Reading Duck focuses exclusively on reading comprehension and literacy development. Every worksheet targets skills like phonics, vocabulary, comprehension, and critical thinking.
This specialized approach aligns with the Science of Reading. Students get systematic, structured practice in the exact skills they need to become better readers. No distractions. No jumping between unrelated topics.
English Worksheets Land covers grammar, writing, speaking, listening, and more. That’s useful for comprehensive language arts instruction. But if your student struggles explicitly with reading comprehension, you’ll spend time sorting through materials that don’t address the core issue.
According to the National Literacy Institute, approximately 40% of students nationwide cannot read at a basic level. When kids struggle this much, they need focused intervention, not scattered practice.
Organization and Ease of Use
Reading Duck organizes worksheets in seven ways:
Grade level (PreK through 12th grade)
Subject (science, language arts, etc.)
Genre (fiction, idioms, expressions)
Word count (20 words to 2,000 words)
Skills (phonics, comprehension, vocabulary)
Holidays (seasonal themes)
Pre-reading activities (foundational preparation)
This flexibility saves time.
Need something for a struggling third grader? Start with grade 2 materials or search by word count.
Want holiday-themed practice? There’s a category for that.
Teaching specific skills? Go straight to the skills section.
English Worksheets Land organizes materials by topic and offers a grade-level sorting option. You’ll find materials on adjectives, adverbs, analogies, and hundreds of other topics arranged by grade from K-12.
However, Reading Duck still offers more flexibility, with 7 organization methods, compared to English Worksheets Land’s two. This means you can search by word count, specific skills, genres, holidays, or pre-reading activities, options that help you quickly match materials to individual student needs beyond just grade and topic.
Why ReadingDuck.com Wins
Feature
ReadingDuck.com
EnglishWorksheetsLand.com
Cost
100% Free
Pricing unclear
Focus
Reading & literacy only
Broad language arts
Organization
7 different ways
Topic-based
Materials
20,000+ worksheets
40,000+ worksheets
Grade Range
PreK-12
Not clearly specified
Registration
None required
May be required
The numbers tell part of the story. Reading Duck removes every barrier between teachers and the materials they need. No cost. No login. No wasted time figuring out which materials match student abilities.
The reading-specific focus matters even more. Every worksheet reinforces literacy skills. Students don’t practice random grammar rules when they need comprehension strategies. They get targeted instruction that builds reading competence step by step.
The multiple organization methods make lesson planning faster. You can search by grade, skill, word count, or any other category that fits your teaching situation. This flexibility helps you meet students where they are and move them forward.
When EnglishWorksheetsLand.com Makes Sense
EnglishWorksheetsLand.com serves a different purpose. If you need comprehensive language arts materials beyond reading, it offers extensive coverage. Grammar instruction, writing practice, speaking activities, and listening exercises all live on one platform.
Teachers managing full English language arts curricula might appreciate having everything in one place. The 40,000+ materials cover nearly every ELA topic you could need.
But for reading instruction specifically, the broad approach creates extra work. You’ll sort through materials to find those that target comprehension, fluency, or vocabulary. That takes time away from actual teaching.
The Final Verdict
EnglishWorksheetsLand.com has its place in comprehensive language arts instruction. But when your goal is improving reading skills, you need a specialized tool. ReadingDuck.com delivers precisely that.
Visit ReadingDuck.com today and explore their 20,000+ free worksheets. Bookmark the site. Share it with fellow educators.
Your students deserve resources that help them succeed without adding costs or complications to your teaching life.
Nursing is one of the most rewarding careers, combining compassion with critical skills to make a real difference in people’s lives. With the demand for nurses expected to grow significantly over the next decade, many aspiring students are eager to enter this noble profession. Yet, the road to becoming a nurse can feel overwhelming, especially when preparing for the rigors of nursing school. Whether you’re making a career shift or pursuing nursing right after college, preparation is the key to success. By understanding what to expect and developing the right strategies, you can set yourself up to thrive in nursing school and beyond.
Understand the Demands of Nursing Programs
Nursing programs, especially an ABSN program, are rigorous and fast-paced. It’s important to know what lies ahead to prepare effectively. Unlike traditional nursing programs that take four years, ABSN programs require a significant time commitment over a shorter period, typically between 11 and 18 months.
This means you’ll need to be ready for full-time coursework, clinical rotations, and long hours of study each day. The workload might feel intense, but knowing what to expect can help you mentally prepare. Talk to current or former students to gain insights into the daily realities of nursing school. Understanding the challenges upfront will make them less daunting when you begin your journey.
Choose a Program That Fits Your Needs
Selecting the right nursing program is critical to your success. Look for a program that aligns with your goals and provides the support you need. Some programs go beyond just teaching and include services like NCLEX licensure preparation and clinical placement assistance.
For example, clinical rotations are a key part of nursing education. These hands-on experiences teach you to apply what you’ve learned in real-world healthcare settings. Programs that help students secure high-quality clinical placements can reduce the stress of finding a preceptor on your own. Additionally, check NCLEX pass rates for the schools you’re considering. A strong pass rate indicates that a program effectively prepares its students for licensure.
Build a Reliable Support Network
Nursing school is challenging, but having a strong support system can make all the difference. Your family, friends, and peers can provide encouragement during stressful times. Faculty and student advisors also play a key role in guiding you through the program.
Many nursing schools offer dedicated student success advisors who work closely with students to help them navigate coursework, clinical schedules, and personal challenges. Developing strong relationships with your instructors is equally important. They can offer valuable insights and mentorship, helping you grow both academically and professionally.
Adopt Smart Study Habits Early
Success in nursing school often depends on how effectively you study. The fast pace of ABSN programs means you need to stay organized and manage your time wisely. Instead of cramming for exams, aim to study consistently every day. Breaking down large topics into smaller sections can make learning more manageable.
Joining a study group can also help. Collaborating with peers allows you to share knowledge, clarify complex concepts, and stay motivated. While group study is useful, remember to set aside individual study time to focus on areas where you need extra practice. Nursing school requires discipline, but with the right habits, you can stay ahead of the curve.
Master Time Management for Success
Time management is a critical skill for nursing students, particularly in accelerated programs. With long hours dedicated to lectures, clinical rotations, and self-study, it’s essential to create a structured schedule. Start by identifying your most productive hours of the day and plan your tasks around them.
Use tools like digital calendars or time-tracking apps to stay on top of assignments and deadlines. Break larger tasks into smaller, more manageable parts to avoid feeling overwhelmed. By setting realistic goals and sticking to a routine, you can effectively balance academics with personal responsibilities. Good time management not only reduces stress but also ensures you stay focused and on track throughout the program.
Prepare Financially for Nursing School
Financial planning is an important step in preparing for nursing school. Tuition, books, and clinical supplies can add up quickly, so it’s essential to budget and explore funding options. Start by researching scholarships and grants specifically for nursing students. Many organizations offer financial assistance to support those entering the field.
If you’re considering student loans, ensure you understand the terms and repayment options. Create a detailed budget to manage your living expenses while in school. Include costs for transportation, meals, and any unexpected expenses. Financial preparedness will allow you to focus on your studies without the added stress of monetary concerns.
Focus on Your Physical and Mental Well-Being
Maintaining your health is crucial for success in nursing school. The demands of the program can take a toll on your physical and mental well-being if you don’t prioritize self-care. Start by establishing a consistent routine that includes a balanced diet, regular exercise, and sufficient sleep.
Incorporate activities that help reduce stress, such as mindfulness or yoga. Spending time with loved ones or engaging in hobbies can also improve your emotional health. Don’t hesitate to seek professional support if you’re feeling overwhelmed. Taking care of yourself ensures you have the energy and resilience needed to handle the challenges of nursing school.
Embrace the Journey with a Positive Mindset
A positive attitude can make all the difference during your nursing school journey. Challenges are inevitable, but viewing them as opportunities to grow will help you stay motivated. Celebrate small achievements along the way, such as mastering a difficult topic or completing a clinical rotation.
Surround yourself with supportive individuals who encourage and inspire you. Focus on your long-term goal of becoming a nurse and the impact you’ll have on patients’ lives. By cultivating a growth mindset, you’ll be better equipped to navigate obstacles and maintain your enthusiasm throughout the program.
Preparing for nursing school requires dedication, planning, and resilience, but the effort is well worth it. By clarifying your goals, choosing the right program, and building strong study habits, you can set a solid foundation for success. Managing your time effectively and prioritizing self-care will ensure you stay focused and healthy throughout the journey.
Remember that challenges are part of the process, but with the right mindset, you can overcome them and thrive. As you embark on this transformative path, know that your preparation today will shape the compassionate and skilled nurse you’ll become tomorrow.
Academic success is a major goal for students, teachers, and parents alike. Whether it’s acing an exam, graduating with honors, or simply doing well in school, understanding what contributes to this success is crucial. While hard work and good study habits are often emphasized, there’s much more beneath the surface. Psychological and biological factors play significant roles in determining a student’s academic achievements. But how do these unseen forces interact to affect learning and performance? Let’s dive deep into both psychological and biological influences to uncover what really drives academic success.
Psychological Factors: Motivation, Mindset, and Emotional Intelligence
When we think of success in school, we often picture motivated students, driven to achieve their goals. Motivation, in fact, is one of the most critical psychological factors influencing academic performance. But motivation isn’t a one-size-fits-all concept. It can be intrinsic, where a student is driven by personal satisfaction, or extrinsic, where external rewards like grades or approval fuel their efforts. Both types of motivation can have a profound effect on how students approach their studies. Sometimes, students may need additional support, such as psychology assignment help, to manage academic pressures and understand complex topics more deeply.
Carol Dweck, a psychologist, popularized the idea of attitude as another important psychological component. While pupils with a fixed mindset feel their IQ is constant, those with a growth mindset think their skills may be enhanced through hard work, according to Dweck. How students respond to difficulties may be impacted by the mentality gap. People who have a growth mentality are more likely to take advantage of educational opportunities, stick with things when they get tough, and eventually do better in school.
Additionally, emotional intelligence (EQ) is crucial. Although IQ has long been used to predict academic success, emotional intelligence—the capacity to recognize and control emotions—had a greater impact on how effectively kids deal with stress, relate to their peers, and recover from failures. A more happy and fruitful learning environment can result from improved coping mechanisms, improved communication, and healthier relationships, all of which are influenced by emotional intelligence.
Cognitive Abilities: Memory, Attention, and Learning Styles
Beyond motivation and mindset, cognitive abilities such as memory, attention, and how we process information are critical for academic success. Have you ever noticed how some students seem to absorb information effortlessly, while others struggle? This often comes down to differences in cognitive functions.
Memory is a key player here, especially working memory, which allows us to hold and manipulate information for short periods. Students with strong working memory can juggle multiple ideas at once, solve complex problems, and retain instructions more easily. Long-term memory also matters—students who can effectively store and retrieve information tend to perform better in subjects that require extensive recall, like history or biology.
Attention is another essential cognitive skill. In a world full of distractions, maintaining focus can be a challenge. Students who struggle with attention may have difficulty following lectures or completing tasks, which impacts their academic outcomes. On the other hand, students who can concentrate for longer periods often absorb more information and complete their work more efficiently.
Each student also has unique learning styles. Some may be visual learners, others auditory, and some may excel through hands-on experiences. Understanding one’s preferred learning style can help optimize study habits and lead to more effective learning. While schools typically employ a one-size-fits-all teaching approach, students who adapt their study methods to align with their personal learning preferences may find greater academic success.
Biological Factors: Genetics, Brain Development, and Sleep
While psychological factors play a significant role in academic success, biology also has a considerable impact. Genetics, for example, can influence a student’s cognitive abilities, such as intelligence, memory capacity, and attention span. While no single gene determines academic success, a combination of genetic factors contributes to a student’s natural aptitude for learning.
The development of the brain also plays a role in academic achievement. During childhood and adolescence, the brain undergoes significant changes that affect cognitive functions. The prefrontal cortex, which is responsible for decision-making, problem-solving, and self-regulation, continues to develop into early adulthood. This means that as students mature, their ability to think critically, plan, and manage their time improves.
One of the most underestimated biological factors influencing academic success is sleep. Studies show that getting enough quality sleep is crucial for memory consolidation, problem-solving, and emotional regulation. Students who are sleep-deprived often experience difficulties with concentration, learning, and coping with stress. With many students juggling heavy workloads and extracurricular activities, sleep often takes a back seat, but its importance cannot be overstated.
The Role of Environment: Nutrition, Physical Activity, and Social Influences
While biological factors such as genetics are beyond our control, other factors, such as environment, can be shaped to support academic success. One of these is nutrition. A well-balanced diet, rich in essential nutrients like omega-3 fatty acids, vitamins, and minerals, is crucial for optimal brain function. Studies have shown that students who eat nutritious meals, particularly breakfast, perform better in school, as they have the energy and focus required for learning.
Physical activity is another environmental factor that influences academic success. Regular exercise has been linked to improved brain function, better mood regulation, and increased focus. In fact, physical activity has been shown to boost the production of brain-derived neurotrophic factor (BDNF), which supports brain health and cognitive development. Students who engage in regular physical activity tend to experience enhanced memory and concentration, leading to better academic outcomes.
Social influences, including family support and peer relationships, also shape academic success. A supportive home environment, where education is prioritized, can motivate students to excel. Similarly, positive peer relationships can encourage academic engagement, while negative influences, such as peer pressure, may lead to poor performance. The social environment a student is exposed to has the power to either lift them up or hold them back.
Interconnection Between Psychological and Biological Factors
While psychological and biological factors can be explored independently, they are deeply interconnected. For instance, a student’s genetic predisposition for attention may influence their ability to stay motivated and focused in class. Similarly, a lack of sleep (a biological factor) can increase emotional instability, making it harder to manage stress or stay motivated (psychological factors). Understanding these interconnections can provide a more holistic view of what drives academic success.
The way these factors interact suggests that boosting academic performance is not just about focusing on one area. Rather, it’s about addressing both the mind and the body—helping students cultivate a positive mindset, supporting cognitive function through sleep and nutrition, and nurturing emotional intelligence. All of these elements work in tandem to create a foundation for academic achievement.
Conclusion
There is much more to academic achievement than skill or hard work. It is the outcome of intricate interactions between biological and psychological elements that affect how well students learn, function, and flourish in educational settings. While cognitive skills like memory and attention influence how well kids learn, motivation, mentality, and emotional intelligence are important psychological components that propel students to achieve. From a biological perspective, sleep, brain development, and genetics are essential for cognitive function and academic achievement. Not to mention the influence of the environment, where elements like social support, physical exercise, and diet provide the educational process additional dimensions. We can better assist students on their path to academic success if we comprehend and handle these elements comprehensively.
Author’s Bio
Matthew Stoll is a skilled content writer with a strong focus on research-driven writing. His expertise lies in creating well-structured essays and academic content, ensuring clarity and precision in every piece. With a deep understanding of various writing styles and formats, Matthew consistently delivers content that meets the specific needs of his audience, from informative articles to comprehensive reports.
Seasoned writers know that the most critical stage of writing academic papers is always editing. While editing, you catch most of the standard mistakes and polish your papers. Properly polished papers often receive much better grades than raw ones because the general neatness of your paper and correct grammar are what most attract the reviewer’s attention.
Suppose you want to create a decent biology research essay, which is a significant paper for your academic performance. In that case, you must dedicate enough time for thorough editing and utilize some effective hacks and tips. We have gathered the most valuable advice for proper proofreading: with our guidance, you will be able to elevate your writing to the next level. If you are still not confident in your abilities to write close-to-perfect papers, contact the science essay writing service for urgent assistance.
Why Proofreading Is So Important
Proofreading is reviewing a work with a critical eye for typos, grammatical mistakes, and punctuation issues. A typical proofreader’s duties include making sure all citations and formatting are consistent and pointing out any instances of ambiguity or misinterpretation. Proper proofreading aids in fixing mistakes such as run-on phrases, fragmented sentences, and comma splices. Little mistakes may slip your mind while you are engrossed in your research and writing. Proofreading is a great way to catch and repair these mistakes.
To be clear, proofreading is not the same as editing. Editing and proofreading are sometimes confused for one another by researchers and PhD candidates. Keep in mind that editing is done before proofreading, and the aim is to make the research paper more explicit by fixing spelling and grammar mistakes and ensuring it is easy to read.
Tips on Proofreading Your Biology Paper
1 – Verify Your Biology Research
Proofreading and editing means not only finding typos and errors in spelling but also applies to finding logical flaws. The most essential part of your biology paper is research, and we recommend starting by rechecking each number and statement from your study. Otherwise, you risk writing the whole paper based on inaccurate facts, which can disaster your academic performance.
2 – Understand the Difference
When you edit your work, you check it for logic, coherence, structure, and argument errors. Grammar, spelling, punctuation, formatting, and consistency are all aspects of a paper that should be carefully examined during proofreading. Editing focuses on the overall structure, whereas proofreading is more concerned with the specifics.
3 – We Recommend Always Starting with Editing
It is standard practice to modify a document first before moving on to proofreading. Doing so can save you the trouble of going back and addressing tiny mistakes that can easily be edited out.
Before you revise your work:
1. Give it a thorough and critical read-through.
2. Make sure it has a clear objective, research question, or hypothesis.
3. Check that the journals and your field’s specific guidelines for paper format and structure are followed.
We also recommend verifying that you have adequately introduced your study topic and provided the necessary background information in your work. Also, check that your work is well-organized and clearly displays your techniques, findings, and discussion. It would also be smart to remember that you need to include credible sources to back up your statements and conclusions throughout the paper and check that the manuscript acknowledges the limitations and consequences of your research.
4 – Listen to Feedback & Use Advanced Writing Tools
When you edit your work, you risk missing typos or weak points in your argument. Because of this, you need to use editing tools and comments to improve your paper. Software or online platforms exist to assist with many aspects of document editing, such as checking for plagiarism, readability, word count, and style. Another option to help you find typical mistakes in your writing is to utilize a grammar or spell checker. On the other hand, you shouldn’t put all your faith in these tools—they may miss inevitable subtle mistakes or details in your paper. The best way to improve your paper is to get comments from people you respect, such as classmates, bosses, or mentors. They will be able to provide you with honest, helpful criticism. Pay attention to their feedback and change your paper based on what they say.
5 – Apply Best Proofreading Techniques
When you proofread your work, you run the risk of missing typos or grammatical mistakes that you’ve grown accustomed to. Use these proofreading approaches to make your work more correct.
To catch typos or strange phrasing you would miss when reading it silently or on your computer, you could print a copy of your paper and read it out loud. Consider reading your paper backward: it will force you to concentrate on the structure and spelling of each word rather than the overall meaning or flow of the sentences. A checklist or guide can remind you what to search for and how to fix any mistakes or inconsistencies in your paper, while a ruler or finger can assist you in avoiding skipping or repeating lines or words.
6 – Double-Check Numbers, References and Symbols
Such mistakes will easily catch the attention of reviewers but can be hard to spot for an average writer. You write this number once at the start and never return to recheck it because you are sure that the stated information is absolutely correct. The standard proofreading practice is double-checking all facts and accurate information in your biology research.
7 – Focus on One Type of Error at a Time
Keep in mind that academic writing proofreading is no picnic. As you go through your text, focus on fixing one typical error type at a time. Checking for spelling, grammar, or punctuation errors could be a good place to start. This method can help you avoid accidentally missing potential mistakes.
The Bottom Line
Writing an excellent biology research essay requires diligence, perseverance, and proper proofreading. We recommend not only looking for spelling errors, but double-checking each number in your final draft and each fact from your study. The outstanding research paper is a balanced combination of accurate information, perfect writing, and impeccable quality, and thorough proofreading can help you guarantee all of these.
Autoimmune mechanisms underline many diseases, some organ-specific, others systemic in distribution.
Autoimmune disorders can overlap: an individual may have more than one organspecific disorder;or more than one systemic disease.
Genetic factors such as HLA type are important in autoimmune disease, and it is probable that each disease involves several factors.
Autoimmune mechanisms are pathogenic in experimental and spontaneous animal models associated with the development of autoimmunity.
Human autoantibodies can be directly pathogenic.
Immune complexes are often associated with systemic autoimmune disease.
Autoreactive B and T cells persist in normal subjects but in disease are selected by autoantigen in the production of autoimmune responses.
Microbial cross-reaching antigens and cytokine dysregulation can lead to autoimmunity.
Autoantibody tests are valuable for diagnosis and sometimes for prognosis.
Treatment of organ-specific diseases usually involves metabolic control. Treatment of systemic diseases includes the use of anti-inflammatory and immunosuppressive drugs.
Future treatment will probably focus on manipulation of the pivotal auto reactive T cells by antigens or peptides, by anti CD4 and possibly T cell vaccination.
THE ASSOCIATION OF AUTOIMMUNITY WITH DISEASE
The immune system has tremendous diversity and because the repertoire of specificities express by the B- and T-cell populations is generated randomly, it is bound to include many which are specific for self components. Thus the body must establish self-tolerance mechanisms, to distinguish between self and non-self determinants, so as to avoid auto reactivity (see Chapter 7). However, al mechanism has a risk of breakdown. The self recognition mechanisms are no exception, and a number of disease have been identified in which there is autoimmunity, due to copious production of autoantibodies and auto reactive T cells. One of the earliest examples in which the production of autoantibodies was associated with disease in a given organ is Hashimoto’s thyroiditis. Among the autoimmune diseases, thyroiditis has been particularly well-studied, and many of the aspects discussed in this chapter will draw upon our knowledge of it. It is a disease of the thyroid which is most common in middle-aged women and often lead to formation of a goiter and hypothyroidism.
The gland is infiltrated, sometimes to an extraordinary extent, with inflammatory lymphoid cells.
These are predominantly mononuclear phagocytes, lymphocytes and plasma cells, and secondary lymphoid follicles are common (Figure-1). In Hashimoto’s disease, the gland often shows regenerating thyroid follicles but this is not a feature of the thyroid in the related condition, primary myxoedema, in which comparable immunology features are seen and where the gland undergoes almost complete destruction and shrinks. The serum of patients with Hashimoto’s disease usually contains antibodies to thyroglobulin. These antibodies are demonstrable by agglutination and by precipitin reactions when present in high titre. Most patients also have anti bodies directed against a cytoplasmic or microsome antigen, also present on the apical surface of the follicular epithelial cells (Figure-2), and now known to be thyroid peroxidase, the enzyme which iodinates thyroglobulin.
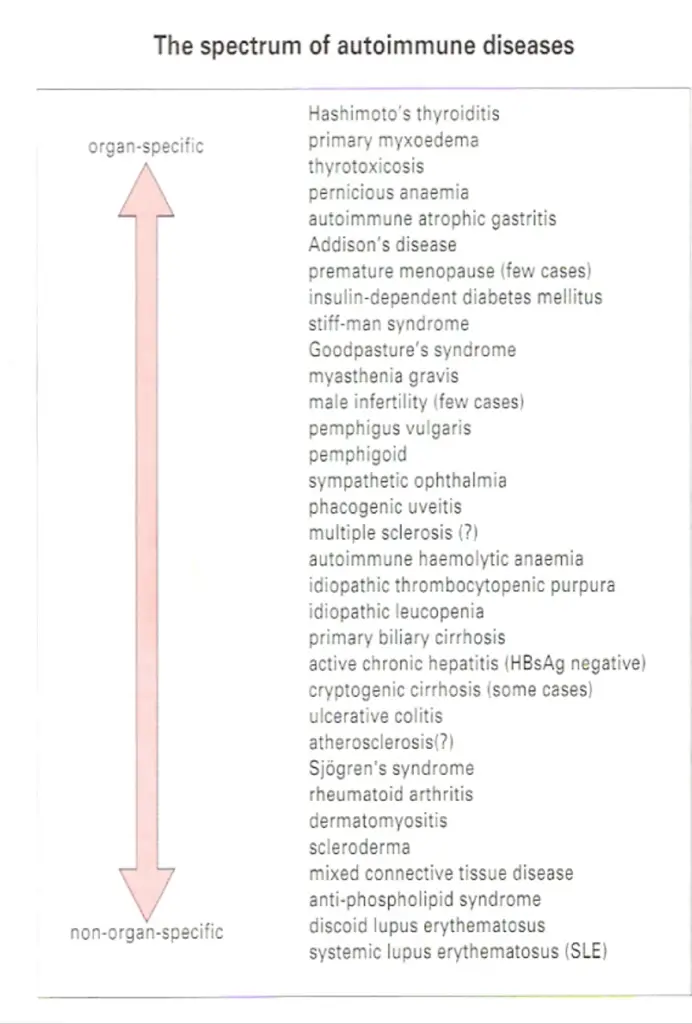
THE SPECTRUM OF AUTOIMMUNE DISEASES
The antibodies associated with Hashimoto’s thyroiditis and primary myxoedema react only with the thyroid, so the resulting lesion is highly localized. By contrast, the serum from patients with diseases such as systemic lupus crythematosus (SLE) reacts with many, if not all, of the tissues I the body. In SLE, one of the dominant antibodies is directed against the cell nucleus (Figure-2). These two diseases represent the extremes of the autoimmune spectrum (Figure-3). The common target organs in organ-specific disease include the thyroid, adrenals, stomach and pancreas. The non-organ-specific diseases, which include the rheumatological disorders, characteristically involve the skin, kidney, joints and muscle (Figure-4).
An individual may have more then one autoimmune disease
Interestingly, there are remarkable overlaps at each end of the spectrum. Thyroid antibodies occur with a high frequency in pernicious anaemia patients who have gastric autoimmunity, and these patients have a higher incidence of thyroid autoimmune disease than the normal population.
Similarly, patients with thyroid autoimmunity have a high incidence of stomach autoantibodies and, to a lesser extent, the clinical disease itself, namely pernicious anaemia. The cluster of hematological disorders at the other end of the spectrum also shows considerable overlap. Features of rheumatoid arthritis, for example, are often associated with the clinical picture of SLE. In these diseases immune complexes are deposited systemically, particularly in the kidney, joints and skin, giving rise to widespread lesions. By contrast, overlap of diseases from the two ends of the spectrum is relatively rare. The mechanisms of immunopathological damage vary depending on where the disease lies in the spectrum. Where the antigen is localized in a particular organ, Type II hypersensitivity and cell-mediated reactions are most important. In non-organ-specific autoimmunity, immune complex deposition leads to inflammation through a variety of mechanisms, including complement activation and phagocyte recruitment.
GENETIC FACTORS
Autoimmune disease can occur in families
There is an undoubted family incidence of autoimmunity. This is largely genetic rather than environmental, as many be seen from studies of identical and non-identical twins, and from the associated of thyroid autoantibodies with abnormalities of the Xchromosome. Within the families of patients with organ-specific autoimmunity, not only is there a general predisposition to develop organ-specific antibodies, it is also clear that other genetically controlled factors tend to select the organ that is mainly affected. Thus, although relatives of Hashimoto patients and families of pernicious anaemia patients both have higher than normal incidence and titer of thyroid autoantibodies, the relatives of pernicious anaemia patients have a far higher frequency of gastric autoantibodies, indicating that there are genetic factors which differentially select the stomach as the target within these families.
Certain HLA Haplotypes Predispose To Autoimmunity
Further evidence for the operation of genetic factors in autoimmune disease comes from their tendency to be associated with particular HLA specificities (Figure-5). Rheumatoid arthritis shows no associations with the HLA-A and-B loci haplotypes, but is associated with a nucleotide sequence (encoding amino acids 70-74 in the DRβ chain) that is common to DR1 and major subtypes of DR4.
This sequence is also present in the dnaJ heat-shock proteins of various bacilli and EBV gp 110 proteins, presenting an interesting possibility for the induction of autoimmunity by a microbial cross-reacting epitope (see below). The plot gets even deeper, though, with the realization that HLA-DR molecules bearing this sequence can bind to another bacterial heat shock protein, dna K, and to the human analogue, namely hsp73, which targets selected proteins to lysosomes for antigen processing. The haplotype B8, DR3 is particularly common in the organ specific diseases, although Hashimoto’s thyroiditis tends to be associated more with DR5. It is notable that for insulin-dependent (type 1) diabetics mellitus, DQ2/8 heterozygotes have a greatly increased risk of developing the disease (Figure-5). Although HLA risk factors tend to dominate-wide searches for mapping the genetic intervals containing genes for predisposition to disease by linkage to micro satellite markers (polymorphic variable numbers of tandem repeats, VNTR) reveal a plethora of genes affecting loss of tolerance, sustained inflammatory responses and end-organ targeting.
Pathogenesis
Autoimmune processes are often pathogenic. When autoantibodies are fond in association with a particular disease there are three possible inferences: • The autoimmunity is responsible for producing the lesions of the disease.
• There is a disease process which, through the production of tissue damage, leads to the development of autoantibodies.
• There is a factor which produces both the lesions and the autoimmunity. Autoantibodies secondary to a lesion (the second possibility) are sometimes found. For example, cardiac autoantibodies may develop after myocardial infarction. However, sustained production of autoantibodies rarely follows the release of autoantigens by simple trauma. In most diseases associated with autoimmunity, the evidence supports the first possibility, that the autoimmune process produces the lesions.
The pathogenic role of autoimmunity can be demonstrated in experimental models
Examples of induced autoimmunity
The most direct test of whether autoimmunity is responsible for the lesions of disease is to induced autoimmunity deliberately in an experimental animal and see if this leads to the production of the lesions. Autoimmunity can be induced in experimental animals by injecting auto antigen (self antigen) together with complete Freund’s adjuvant, and this does indeed produce organ-specific disease in certain organs. For example, thyroglobulin injection can induce an inflammatory disease of the thyroid while myelin basic protein can cause encephalomyelitis. In the case of thyroglobulin-injected animals, not only are thyroid autoantibodies produced, but the gland becomes infiltrated with mononuclear cells and the acinar architecture crumbles, closely resembling the histology of Hashimoto’s thyroiditis. The ability to induce experimental autoimmune disease depends on the strain of animal used.
For example, it is found that the susceptibility of rats and mice to myelin basic protein-induced encephalomyelitis depends on a small number of gene loci, of which the most important are the MHC class II genes. The disease can be induced in susceptible strains by injecting T cells belong to the CD4/TH1 subset and it has been found that induction of disease can be prevented by treating the recipients with antibody to CD4 just before the expected time of disease onset, blocking the interaction of the TH cells’ CD4 with the class II MHC of antigen-presenting target cells. The results indicate the importance of class II restricted auto reactive TH cells I the development of these conditions, and emphasize the prominent role of the MHC.
Examples of spontaneous autoimmunity
It has proved possible to breed strains to animals which are genetically programmed to develop autoimmune diseases closely resembling their human counterparts. One well established example is the Obese strain (OS) chicken (Figure-6) which parallels human autoimmune thyroid disease in terms of the lesion in the gland, the production of antibodies to different components in the thyroid, and the overlap with gastric autoimmunity. So it is of interest that when the immunological status of these animals is altered, quite dramatic effects on the outcome of the disease are seen.
For example, removal of the thymus at birth appears to exacerbate the thyroiditis, suggesting that the thymus exerts a controlling effect on the disease, but if the entire T-cell population is abrogated by combining thymectomy with massive injections of anti-chick T-cell serum, both autoantibody production and the attack on thyroid are completely inhibited. Thus, T cells play a variety of pivotal roles as mediators and regulators of this disease. The non-obese diabetic (NOD) mouse provides an excellent model for human insulin-dependent diabetes mellitus (IDDM; type 1 diabetes) where the insulin producing β cells of the pancreatic islets of Langerhans are under attack from a chronic leukocytic infiltrate of T cells and macrophages (Figure-7). The role of the T cells in mediating this attack is evident from the amelioration and prevention of disease by treatment of the mice with a non-depending anti-CD4 monoclonal antibody, which in the presence of the pancreatic auto-antigens, insulin and glutamic acid decarboxylase (GAD) induces specific T cell anergy. The dependence of yet another spontaneous model, the F1 hybrid of New Zealand Black and White strains (NZB x W/F1), on the operation of immunological processes is aptly revealed by the suppression of the murine SLE which characterizes this strain, by treatment with anti-CD4 (Figure-8).
Human autoantibodies can be directly pathogenic
When investigating human autoimmunity directly, rather than using animal models, it is of course more difficult to carry out experiments. Nevertheless, there is much evidence to suggest that autoantibodies may be important in pathogenesis, and we will discuss the major examples here.
Thyroid autoimmune disease – A number of disease have been recognized in which autoantibodies to hormone receptors may actually mimic the function of the normal hormone concerned and produce disease. Graves’ disease (thyrotoxicosis) was the first disorder in which such anti-receptor antibodies were clearly recognized. The phenomenon of neonatal thyrotoxicosis provides us with a natural ‘passive transfer’ study, because the IgG antibodies from the thyrotoxic mother cross the placenta and react directly with thyroid stimulating hormone (TSH) receptor o the neonatal thyroid.
Many babies born to thyrotoxic mothers and showing thyroid hyperactivity have been reported, but the problem spontaneously resolves as the antibodies derived from the mother are catabolized in the baby over several weeks. Whereas autoantibodies to the TSH receptor may stimulate cell division and/or increase the production of thyroid hormones, others can bring about the opposite effect by inhibiting these functions, a phenomenon frequently observed in the receptor responses to ligands which act as agonists or antagonists. Different combinations of the various manifestations of thyroid autoimmune disease, chronic inflammatory cell destruction and stimulation or inhibition of growth and thyroid hormone synthesis, can give rise to a wide spectrum of clinical thyroid dysfunction (Figure-9).
Myasthenia gravis – A parallel with neonatal hyperthyroidism has been observed with mothers suffering from myasthenia gravis, where antibodies to acetylcholine receptors cross the placenta into the fetus and may cause transient muscle weakness in the newborn baby.
Other receptor diseases – Somewhat rarely, autoantibodies to insulin receptors and to βadrenergic receptors can be found, the latter associated with bronchial asthma. Neuromuscular defects can be elicited in mice injected with serum from patients with the Lambert – Eaton syndrome containing antibodies to presynaptic calcium channels, while sodium channel autoantibodies have been identified in the Guillain – Barre syndrome.
Male infertility – Yet another example of autoimmune disease is seen in rate cases of male infertility were antibodies to spermatozoa lead to clumping of spermatozoa, either by their heads or by their tails, in the semen.
Pernicious anaemia – In this disease an autoantibody interferes with the normal uptake of vitamin B12.Vitamine B12 is not absorbed directly, but must first associated with a protein called intrinsic factor; the vitamin-protein complex is then transported across the intestinal mucosa. Early passive transfer studies demonstrated that serum from a patient with pernicious anaemia, if fed to a healthy individual together with intrinsic factor – B12 complex, inhibited uptake of the vitamin.
Subsequently, the factor in the serum which blocked vitamin uptake was identified as antibody against intrinsic factor. It is now known that plasma cells in the gastric mucosa of patients with pernicious anaemia secrete this antibody into the lumen of the stomach (Figure-10).
Goodpasture’s syndrome – In goodpasture’s syndrome, antibodies to the glomerular capillary basement membrane bind to the kidney in vivo (Figure-3). To demonstrate that the antibodies can have a pathological effect, a passive transfer experiment was performed. The antibodies were eluted from the kidney of a patient who had died with this disease, and injected into primates whose kidney antigens were sufficiently similar for the injected antibodies to localize on the glomerular basement membrane. The injected monkeys subsequently died with glomerulonephritis.
Blood and vascular disorders – Autoimmune haemolytic anaemia and idiopathic thrombocytopenia purpura result from the synthesis of autoantibodies to red cells and platelets, respectively. The primary antiphospholipid syndrome characterized by recurrent thromboembolic phenomena and feta loss is triggered by the reaction of autoantibodies with a complex of β2-glycoprotein turns up again as an abundant component of atherosclerotic plaques and there is increasing attention to the idea that autoimmunity may initiate or exacerbate the process of lipid deposition and plaque formation in this disease, the two lead candidate antigens being heat-shock protein 60 and the low- density lipoprotein, apoprotein B. The necrotizing granulomatous vasculitis which characterizes Wegener’s granulomatosis is associated with antibodies to neutrophil cytoplasmic proteinase III (cANCA) but their role in pathogenesis of the vaculitis is ill defined.
Immune Complexes appear to be pathogenic in systemic autoimmunity
In the case of SLE, it can be shown that complement-fixing complexes of antibody with DNA and other nucleosome components such as histones are deposited in the kidney (Figure-3), skin, joints and choroid plexus of patients, and must be presumed to produce Type III hypersensitivity reactions. Cationic anti-DNA antibodies and histones facilitate the binding to heparin sulphate in the connective tissue structures. Individuals with genetic deficiency of the early classical pathway complement components clear circulating immune complexes very poorly and are unduly susceptible to the development of SLE. Turing to the experimental models, we have already mentioned the (NZB x W) F1 which spontaneously develops murine SLE associated with immune-complex glomerulonephritis and anti-DNA autoantibodies as major features. The fact that measures which suppress the immune response in these animals (e.g. treatment with azathioprine or anit-CD4) also suppress the disease and prolong survival, adds to the evidence for autoimmune reactions causing such disease (Figure-8).
The erosions of cartilage and bone in rheumatoid arthritis are mediated by macrophages and fibroblasts which become stimulated by cytokines from activated T cells and immune complexes generated by a vigorous immunological reaction within the synovial tissue. The complexes can arise through the self-association of IgG rheumatoid factors specific for the Fcy domains, a process facilitated by the striking deficiency of terminal galactose on the biantennary N-linked Fc iligosaccharides (Figure-11). This agalacto glycoform of IgG in complexes can exacerbate inflammatory reactions through reaction with mannosebinding lectin and production of TNE.
Evidence for directly pathogenic T cells in human autoimmune disease is hard to get
Adoptive transfer studies have shown that TH1 cells are responsible for directly initiating the lesions in experimental models of organ-specific autoimmunity. In the human, the production of high affinity, somatically mutated IgG autoantibodies characteristic of Tdependent responses, the isolation of thyroid-specific T-cell clones from the glands of Graves’ disease patients, the beneficial effect of cyclosporine in pre-diabetic individuals and the close association with certain HLA haplotypes, make it abundantly clear that T cells are utterly pivotal for the development of autoimmune disease. However, it is difficult to identify a role for the T cell as a pathogenic agent as distinct from a T-helper function in the organ-specific disorders. Indirect evidence from circumstances showing that antibodies themselves do not cause disease, such as in babies born to mothers with insulin-dependent diabetes (IDDM), may be indicative.
Autoimmunity is antigen driven
Given that auto-reactive B cells exist, the question remains whether they are stimulated to proliferate and produce autoantibodies by interaction with auto-antigens or by some other means, such as non-specific polyclonal activators or idiotypic interactions (Figure-14). Evidence that B cells are selected by antigen comes from the existence of high affinity autoantibodies which arise through somatic mutation, a process which requires both T cells and autoantigen.
Additionally, autoantibodies to epitope clusters occur on the same auto-antigenic molecule. Apart from the presence of auto-antigen itself, it is very difficult to envisage a mechanism that could account for the co-existence of antibody responses to different epitopes on the same molecule. A similar argument applies to the induction, in a single individual, of autoantibodies to organcelles (e.g. nucleosomes and spliceosomes which appear as belbs on the surface of apoptotic cells) or antigens linked within the same organ (e.g. thyroglobulin and thyroid peroxidase).
The most direct evidence for autoimmunity being antigen driven comes from studies of the Obese strain chicken which, as described earlier, spontaneously develops thyroid autoimmunity. If the thyroid gland (the source of antigen) is removed at birth, the chickens mature without developing thyroid autoantibodies (Figure-13). Furthermore, once thyroid autoimmunity has developed, later removal of the thyroid leads to a gross decline of thyroid autoantibodies, usually to undetectable levels. Comparable experiments have been carried out in the non-obese diabetic (NOD) mouse which models human autoimmune diabetes; chemical destruction of the β cells leads to decline in pancreatic autoantibodies. DNase treatment of lupus mice ameliorates the disease, presumably by destroying potentially pathogenic immune complexes.
In organ-specific disorders, there is ample evidence for T cells responding to antigens present in the organs under attack. But in non-organ-specific autoimmunity, identification of the antigens recognized by T cells is often inadequate. True, histone-specific T cells are generated in SLE patients and histone could pay a ‘piggy back’ role in the formation of anti-DNA antibodies by substituting for natural antibody in the mechanism outlined in Figure-14. Another possibility is that the T cells do not see conventional peptide antigen (possibly true of anit-DNA responses) but instead recognize an antibody’s idiotype (an antigenic determinant on the V region of antibody). In this view SLE, for example, might sometimes be initiated as an ‘idiotype disease’, like the model presented in Figure-14 In this scheme, autoantibodies are produced normally at low levels by B cells using germ-line genes. If these then form complexes with the autoantigen, the complexes can be taken up by APCs (including B cells) and components of the complex, including the antibody idiotype, presented to T cells. Idiotype-specific T cells would then help the autoantibody-producing B cells. Evidence for the induction of anti-DNA and glomerulonephritis by immunization of mice with the idiotype of germ-line ‘natural’ antiDNA autoantibody lends credence to this hypothesis.
Controls on the development of autoimmunity can be bypassed in a number of ways
Molecular mimicry by cross-reactive microbial antigens can stimulate autoreactive B and T cells
Normally, naïve autoreactive T cells recognizing cryptic self epitopes are not switched on because the antigen is only presented at low concentrations on ‘professional’ APCs or it may bepresented on ‘non-professional’ APCs such as pancreatic β-islet cells or thyroid epithelial cells, which lack B7 or other co-stimulator molecules. However, infection with a microbe bearing antigens that cross-react with the cryptic self epitopes (i.e. have shared epitopes) will load the professional APCs with levels of processed peptides that are sufficient to activate the naïve autoreactive T cells. Once primed, these T cells are able to recognize and react with the self epitope on the non-professional APCs since they no longer require a co-stimulatory signal and have a higher avidity for the target, due to upregulationof accessory adhesion molecules (Figure-15).
Cross reactive antigens which share B cell epitopes with self molecules can also break tolerance but by a different mechanism. Many autoreactive B cells cannot be activated because the CD4+ helper T cells which they need are unresponsive either because these helper T cells are tolerized at lower concentration of autoantigens than the B cells or because they only recognize cryptic epitopes. However, these ‘helpless’ B cells can be stimulated if the cross-reaching antigen bears a ‘foreign’ carrier epitope to which the T cells have not been tolerized (Figure-16). The autoimmune process may persist after clearance of the foreign antigen if the activated B cells now focus the autoantigen on their surface receptors and present it to normally resting autoreactive T cell which will then proliferate and act as helpers for fresh B-cell stimulation.
A disease in which such molecular mimicry operates is rheumatic fever, in which autoantibodies to heart valve antigen can be detected. These develop in a small proportion of individuals several weeks after a streptococcal infection of the throat. Carbohydrate antigens on the streptococci cross-react with an antigen on heart valves, so the infection may bypass T-cell self tolerance to heart valve antigens. Shared B-cell epitopes between Yersinia enterolytica and the extracellular domain of the TSH receptor have recently been described. There may also be cross reactivity between HLA-B27 and certain strains of Klebsiella in connection with ankylosing spondylitis, and crossreactivity between bacterial heat-shock proteins and DR4 in relationship to rheumatoid arthritis.
In this connection, it has been suggested that because processed MHC molecules may represent a major fraction of the peptide emitopes presented to differentiating T cells within the thymus, a significant proportion of positively selected cell which escape negative selection and enter the periphery will be specific for weakly binding cryptic MHC epitopes. One might therefore expect autoimmune responses to arise not infrequently through activation of these cells by molecular mimicry.
In some cases foreign antigen can directly stimulate auto-reactive cells
Another mechanism to bypass the tolerant autoreactive TH cell is where antigen or another stimulator directly triggers the autoreactive effector cells. For example, lipopolysaccharide or Epstein-Barr virus causes direct B-cell stimulation and some of the clones of activated cells will produce autoantibodies, although in the absence of T-cell help these are normally of low titer and affinity. However, it is conceivable that an activated B cell might pick up and process its cognate autoantigen and present it to a naïve autoreactive T cell.
Cytokine dysregulation, inappropriate MHC expression and failure of suppression may induce autoimmunity
It appears that dysregulation of the cytokine network can also lead to activation of autoreactive T cells. One experimental demonstration of this is the introduction of a transgene for interferon-γ (IFNγ) into pancreatic β-islet cells. If the transgene for IFNγ is fully expressed in the cells, MHC class II genes are upregulated and autoimmune destruction of the islet cell results (Figure-17). This is not simply a result of a nonspecific chaotic IFNγ-induced local inflammatory milieu since normal islets grafted at a separate site are rejected, implying clearly that T-cell autoreactivity to the pancreas has been established.
The surface expression of MHC class II in itself is not sufficient to activate the naïve autoreactive T cells but it may be necessary to allow a cell to act as a target for the primed autoreactive TH cells, and it was therefore most exciting when cells taken from the glands of patients with Graves’ disease were found to be actively synthesizing class II MHC molecules (Figure-18) and so were able to be recognized by CD4+ T cells. In this context it is interesting that isolated cells from several animal strains that are susceptible to autoimmunity are also more readily induced by IFNγ to express MHC class II than are cells from non-susceptible strains.
The argument that imbalanced cytokine production may also contribute to autoimmunity receives further support from the unexpected finding that tumour necrosis factor (introduced by means of a TNF transgene) ameliorates autoimmune disease in NZB x NZW hybrid mice.
Aside from the normal ‘ignorance’ of cryptic self-epitopes, other factors which normally restrain potentially autoreactive cells may include regulatory T cells, hormones (e.g. steroids), cytokines (e.g. TGFβ) and products of macrophages (Figure-19). Deficiencies in any of them may increase susceptibility to autoimmunity. The feedback loop on Thelpersand macrophages through the pituitary – adrental axis is particularly interesting, as defects at different stages in the loop turn up in a variety of autoimmune disorders Figure-20). For example, patients with rheumatoid arthritis have low circulating corticosteroid levels compared with controls, and after surgery, although they produce copious amounts of IL-1
and IL-6, a defect in the hypothalamic paraventricular nucleus prevents the expected increase in ACTH and adrenal steroid output. A subset of CD4 regulatory cell present in young healthy mice of the NOD strain can prevent the transfer of disease by spleen cells of diabetic animals to NOD mice congenic for the severe combined immunodeficiency trait; this regulatory subset is lost in older mice.
Pre-existing defects in the target organ may increase susceptibility to autoimmunity
We have already alluded to the undue sensitivity of target cells to upregulation of MHC class II by IFNγ in animals susceptible to certain autoimmune disease: Other evidence also favours the view that there may be a pre-existing defect in the target organ. In the Obese strain chicken model of spontaneous thyroid autoimmunity, not only is there a low threshold of IFNγ induction of MHC class II expressin by thyrocytes but it has also been shown that, when endogenous TSH is suppressed by thyroxine treatment, the uptake of iodine into the thyroid glands is far higher in the Obese strain than in a variety of normal strains. Furthermore, this is not due to any stimulating animals show even higher uptakes of iodine (Figure-21). Interestingly, the Cornell strain (from which the Obese strain was derived by breeding) shows even higher uptakes of iodine, yet these animals do not develop spontaneous thyroiditis. This could be indicative of a type of abnormal thyroid behavior which in itself is insufficient to induce autoimmune disease but does contribute to susceptibility in the Obese strain. Other situations in which the production of autoantigen is affected are diabetes, in which one of the genetic risk factors is associated with a microsatellite marker lying within a transcription factor controlling the rate of insulin production, and rheumatoid arthritis, in which the agalacto IgG glycoform is abnormally abundant. The intriguing observations that immunization atherosclerotic lesions at classical predilection sites object to major haemodynamic stress and that patients with atherosclerosis produce antibodies to human hsp60 which react with heat or IFNα-stressed endothelial cells, hints strongly at an autoimmune contribution to the pathology of the disease. Particularly relevant to the present discussion is the finding of upregulated hasp60 expression at such critical sites even in a 5-month-old child (Figure22). Again, one must re-emphasize the considerable importance of multiple factors I the establishment of prolonged autoimmunity.
DIAGONOSTIC AND PROGNOSTIC VALUE OF AUTOANTIBODIES
Wherever the relationship of autoantibodies to the disease process, they frequently provide valuable markers for diagnostic purposes. A particularly good example is the test for mitochondrial antibodies, used in diagnosing primary biliary cirrhosis (Figure-23). Exploratory laparotomy was previously needed to obtain this diagnosis, and was often hazardous because of the age and condition of the patients concerned. Autoantibodies often have predictive value. For instance, individuals testing positively for antibodies to both insulin and glutamic acid decarboxylase have a high risk of developing insulin-dependent diabetes.
TREATMENT
Often, in organ-specific autoimmune disorders, the symptoms can be conrolled by administration of thyroxine, and thyrotoxicosis by antithyroid drugs. In pernicious anaemia,
metabolic correction is achieved by injection of vitamin B12, and in myasthenia gravis by administration of cholinesterase inhibitors. If the target organ is not completely destroyed, it may be possible to protect the surviving cells by transfection with FasL or TGFβ genes. Where function is completely lost and cannot be substituted by hormones, as many occur in lupus nephritis or chronic rheumatoid arthritis, tissue grafts or mechanical substitutes may be appropriate. In the case of tissue grafts, protection from the immunological processes which necessitated the transplant may be required.
Conventional immunosuppressive therapy with antimitotic drugs at high doses can be used to dam down the immune response but, because of the dangers involved, tends to be used only in life-threatening disorders such as SLE and dermatomyositis. The potential of cyclosporine and related drugs such as rapamycin has yet to be fully realized, but quite dramatic results have been reported in the treatment of type 1 diabetes mellitus. Anitinflammatory drugs are, of course, prescribed for rheumatoid diseases with the introduction of selective cyclo-oxygenase-2 (COX-2) inhibitors representing a welcome development. Encouraging results are being obtained by treatment of rheumatoid arthritis patients with low steroid doses at an early stage to correct the apparently defective production of these corticosteroids by the adrenal feedback loop, and for those with more established disease, attention is now focused on the striking remissions achieved by synergistic treatment with anti-TNFα monoclonals plus methotrexate.
As we understand more about the precise defects, and learn how to manipulate the immunological status of the patient, some less well-established approaches may become practicable (Figure-24). Several centres are trying out autologous stem-cell transplantation following haemato-immunoablation with cytotoxic drugs in severe cases of SLE, scleroderma and rheumatoid arthritis. Draconian reduction in the T cells in multiple sclerosis by Campath-1H (anti-CD52) and of the B-cell population with antiCD20 in rheumatoid arthritis are both under scrutiny. Treatment with Campath-1H followed by a non-depleting anti-CD4 has produced excellent remissions in patients with Wegener’s granulomatosis who were refractory to normal treatment. In an attempt to establish antigenspecific suppression, considerable clinical improvement has been achieved in exacerbating remitting multiple sclerosis by repeated injection of Cop 1, a random copolymer of alanine, glutamic acid, lysine and tyrosine meant to simulate the postulated ‘guilty’ autoantigen, myelin basic protection. Some experimental autoimmune disease have been treated successfully by feeding antigen to induce oral tolerance, by the inhalation of autoantigenic peptides and their analogues (Figure-25), and by ‘vaccination’ with peptides from heat-shock protein 70 or the antigen-specific receptor or autoreactive T cells. This suggests that stimulating normally suppressive functions, including the idiotype network, could be promising.
CRITICAL THINKING: Autoimmunity and autoimmune disease
Miss Jacob, a 30-year-old Caribbean lady, was seen in a rheumatology clinic with stiff painful joints in her hands, which were worse first thing in the morning. Other symptoms included fatigue, a low-grade fever, a weight loss of 2 kg, and some mild chest pain. Miss Jacob had recently returned to the UK from a holiday in Jamaica and was also noted to be taking the combined oral contraceptive pill. Past medical history of note was a mild autoimmune haemolytic anaemia 2 years previously. On examination Miss Jacob had a non-specific maculopapular rash on her face and chest and patchy alopecia (hair loss) over her scalp. Her mouth was tender and examination revealed an ulcer on the soft palate. She had moderately swollen and tender proximal interphalangeal joints. Her other joints were unaffected, but she had generalized muscle aches. The results of investigations are shown in Figure-26.